Mary E. Hanley DO, MBA, UHM, CWSP, FAPWCA
Medical Director, Wound, Vascular, and Hyperbaric Medicine. Roper St. Francis Healthcare, Charleston, SC USA
Introduction
Antibiotic resistant infections in chronic wounds is a growing worldwide problem. PreventogenTM polymer is a topical liquid applied to wound beds to decrease biofilm, kill bacteria and promote healing.
- 7 to 8 Million people currently live with chronic wounds in the US, nearly 2.5% of the population1
- Numbers expected to rise as population ages
- Type II Diabetes and Obesity epidemics in the US and worldwide add to the problem
- 26.4 per 1000 hospital inpatients have chronic wounds on admission in the US2
- Estimated annual cost for chronic wound management in the USA ranges from $28.1 to $96.8 billion3
By 2050, 10,000,000 people will die every year due to antimicrobial resistance (AMR)
Up to 33% of surgical patients get a postoperative infection, of which 51% can be antibiotic resistant
Surgical site infections (SSIs) are amongst the most common healthcare-associated infections (20% of all HAIs)
Staphylococcus aureus (MRSA) is the most common microbial cause
Materials
20 patients (16 male, 4 female, average age 64) were randomly assigned to either standard of care (SOC), which consisted of weekly visits, debridement, MedCUTM copper foam dressings, offloading, or standard of care plus PreventogenTM polymer applied to the wound bed post debridement. (SOC +). Patients were followed until wound closure was achieved. Patients had either Wagner 2 or Wagner 3 Diabetic foot ulcers on the plantar surface of the foot.
Methods
Patients were seen weekly in multidisciplinary limb preservation clinic. Wound size was measured at every visit. Presence of infection, such as odor, increased drainage, fluctuance, periwound induration, lymphangitis, fever > 38°C were noted. Need for systemic antibiotic therapy was noted. None of the patients in the SOC+ group, required systemic antibiotic therapy during the course of treatment, whereas 6 patients in the SOC group (60%) did require systemic (oral) antibiotic therapy during the course of their wound care treatment. Biofilm formation was observed to be less in the SOC+ group as well as evidenced by less need for selective or excisional debridement. Increased granulation tissue formation was noted in the SOC+ group as evidenced by faster healing time. There were no adverse effects or complications noted in the SOC+ group.
Results
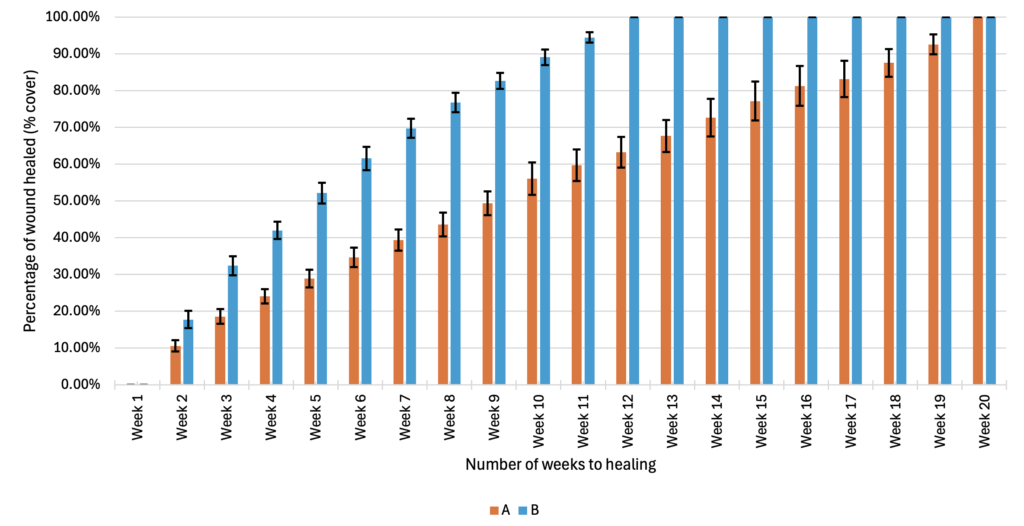
By week 12 the SOC+ group had healed completely. The SOC group healed by week 20. This was a statistically significant difference. Patients treated with PreventogenTM polymer in addition to SOC showed faster time to healing with less incidence or observed wound infection needing treatment with systemic antibiotics.
Conclusion
Diabetic foot ulcers are a serious, potentially life and limb threatening condition leading to amputation and permanent disability. Treating them aggressively but without the need for systemic antibiotics is a new paradigm made possible by the use of PreventogenTM polymer. Use of this polymer can decrease the incidence of wound infection and the need for systemic antibiotics who’s use can contribute to antibiotic resistance and other complications related to antibiotic therapy. Healing these complex wounds with fewer systemic antibiotics in a shorter span of time can save lives and limbs.
